For Clinicians
The SELECT Trial - A New Era in Obesity and Cardiovascular Care
The landmark SELECT trial shows semaglutide reduces heart attacks, strokes, and death — reshaping obesity treatment forever.

Semaglutide's ability to reduce heart attacks and strokes
Today, I am diving into the SELECT Semaglutide Trial (also known as Ozempic and Wegoy) that was just released at the AHA annual conference and published in the New England Journal of Medicine. This is a groundbreaking study that will reshape our approach to obesity and cardiovascular health. The intervention was done on top of routine standard care so it tells us a lot more about real world impacts of semaglutide and future obesity medications. It's about real people, real health, and the future of obesity treatment. As an obesity physician with a heart for holistic care, here are my top takeaways from this landmark study.A Game-Changer for Cardiovascular Risk and Mortality
The SELECT trial showed a 1.5% absolute and a 20% relative risk reduction in cardiovascular death, non-fatal MI, and non-fatal stroke. For context, that's a huge leap forward in heart health. It mirrors the impact we have seen from statins, ace inhibitors, and beta-blockers in similar populations and generally those studies have had a longer treatment duration meaning that semaglutide could be a far superior intervention at the 5 year mark. To clarify, the study was done on people with a history of cardiovascular disease. We still do not know if we would get similar risk reduction in people struggling with obesity who do not have a history of heart disease or diabetes.Surprise Finding: A Decrease in All-Cause Mortality
The trial showed a 19% reduction in all-cause mortality in three years. I think this is a big deal over a 3 year window. It’s on par with the 3 year risk mortality reduction seen in bariatric surgery. In bariatric surgery all cause mortality decreases by 50% over 10 years. Imagine if the mortality benefit of semaglutide continues to expand over 10 years and we can deliver this intervention at scale. Preventive healthcare could vastly change and one could make an argument that incretins(GLP-1s) could be a greater disruptive force in healthcare than AI. We still have a long way to go before we get there. For us to consider medication-driven obesity treatments as equivalent to bariatric surgery, it's essential that they demonstrate mortality benefits across all obesity patients, including those who do not have cardiovascular disease or diabetes.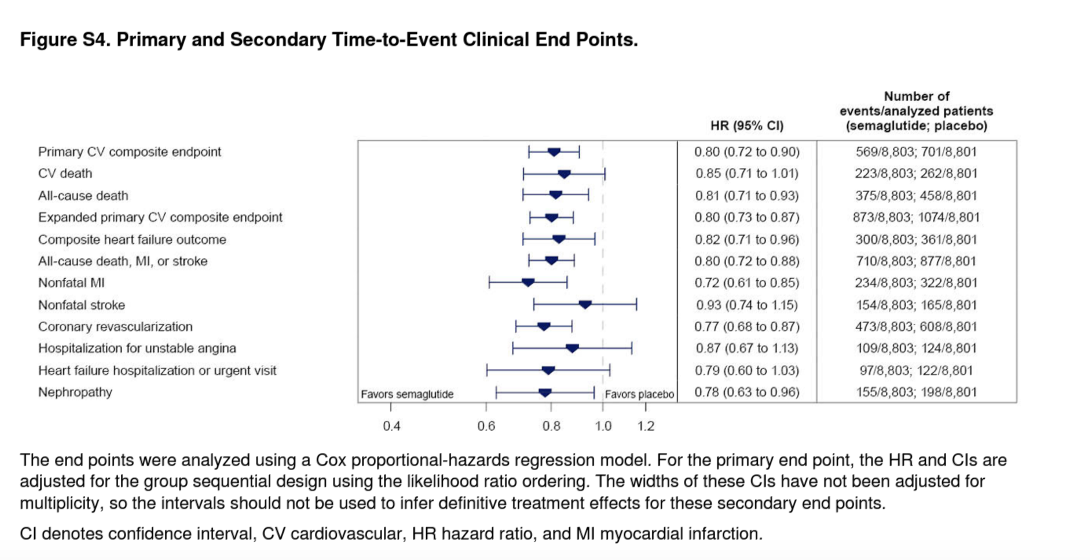
Real world, Real People, Less Weight Loss
Why was weight loss less in the Select Trials? The weight loss in the SELECT trial ( –9.39%) was 35% less than weight loss delivered in semaglutide’s STEP 1 trial (–14.9%). Many people are perplexed by this but I would argue that this trial represents what we should expect from Semaglutide in our day to day practice. The SELECT trial reflects the real world - older, diverse participants, and in usual care settings without lifestyle and behavioral support. Some specific data points:- SELECT participants were older (average age 61 vs. 47 in STEP 1), predominantly male (72% vs. 27%), and had a lower average BMI (33 vs. 38).
- SELECT added Semaglutide to standard care. Whereas the STEP 1 trial delivered semaglutide with wrap around care. In STEP 1, participants engaged in 16 intensive lifestyle and behavioral counseling sessions and monitored and tracked their food and exercise.
- The STEP 1 excluded individuals with a history of major depressive disorder within two years(many likely on weight gaining medications), history of substance abuse, significant weight change (> 5 kg) within 90 days. In contrast, SELECT had a more inclusive approach, reflecting a broader and real world patient population.
- A notable 70.2% of SELECT participants were on beta-blockers, which can affect weight loss. This aspect is crucial for understanding the varied outcomes between the trials. I am curious to see what the average weight loss was for 30% of individuals that were not on beta blocker.
The Outcome I Wanted To See But Did Not
The placebo and treatment group in the SELECT trial showed similar cancer rates (4.7% and 4.8%,respectively). Unlike cardiovascular outcomes, these findings diverge from studies showing up to a 40% cancer rate reduction with bariatric surgery. The study may be underpowered and to short to detect changes in cancer rates. Regardless, we should ask why we see cancer reduction with bariatric surgery that we are not yet witnessing with GLP-1 driven weight loss. It's worth noting that in lifestyle based weight loss, we do see a modest 16% decrease in obesity related cancer but not all cancer. A subanalysis of the SELECT trial on obesity related cancer incidence would be fascinating.Wrapping it up
The SELECT trial is more than a study; it's a window into the possibilities in obesity and cardiovascular treatment. As a physician dedicated to holistic care, I view Semaglutide as an essential component, but not the complete solution. The differences in weight loss between SELECT and STEP I highlight the crucial role of comprehensive care beyond medication. Embracing the complexity of obesity treatment means understanding the whole person – their lifestyle, challenges, and goals. As physicians and clinics consider using Semaglutide to reduce risk and disease, it's equally important to invest in lifestyle and behavioral support. At Enara, we partner with clinics and physicians to scale holistic care models, ensuring that treatment is not just about prescribing medication, but about nurturing the entire spectrum of patient health and well-being.