Hybrid Obesity Care Reduces Inflammation at 12 Months in Adults With Obesity
- Enara Health , San Mateo, CA, USA
Background
Chronic inflammation contributes to cardiometabolic risk in adults with obesity. High-sensitivity C-reactive protein (hsCRP) is a clinically relevant biomarker of systemic inflammation that can improve with effective obesity care. Hybrid medical weight-management programs combine lifestyle, behavioral, and optional pharmacologic interventions to support long-term health. Real-world data on inflammatory outcomes in these programs are limited. This study evaluates hsCRP trajectories at 3, 6, and 12 months among adults participating in a hybrid obesity program, comparing those receiving anti-obesity medications (AOMs) with those managed through lifestyle and behavioral interventions alone.
Methods
This retrospective cohort analysis included 355 adults with BMI ≥30 kg/m² enrolled for 12 months in a hybrid digital–clinic obesity program. Participants were grouped by AOM use versus non-AOM care. Inclusion required baseline hsCRP and at least one follow-up measurement at 3, 6, or 12 months. hsCRP and weight were measured at each timepoint. Change in hsCRP from baseline was calculated for 3, 6, and 12 months. Descriptive statistics (mean, median, SD, n) were summarized, and approximate independent t-tests were performed for group comparisons at each timepoint.
Results
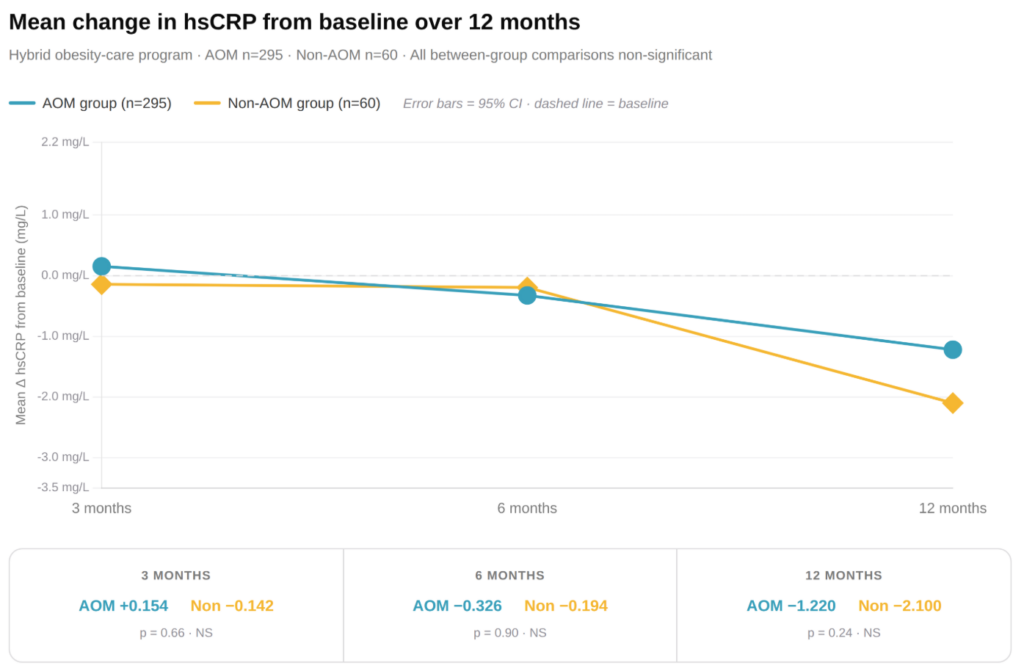
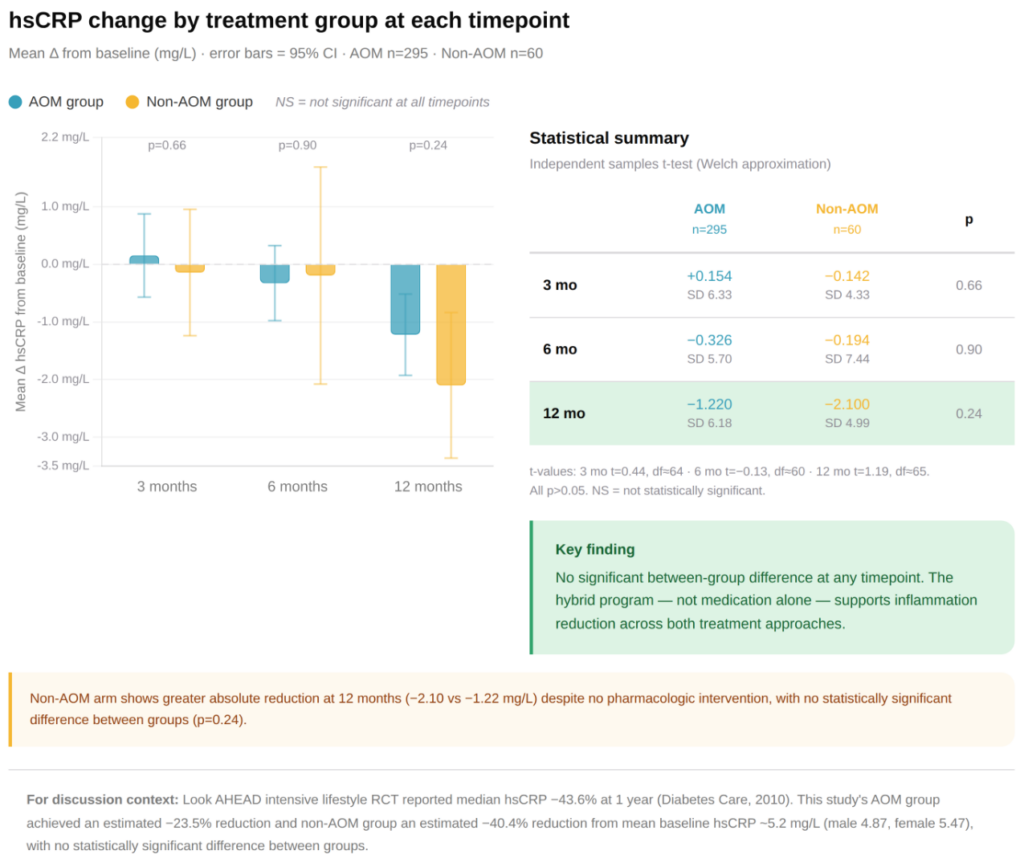
Both AOM (n=295) and non-AOM (n=60) participants demonstrated reductions in hsCRP at 12 months, indicating decreased systemic inflammation with hybrid program participation. Mean change at 12 months was –1.22 mg/L (SD 6.18) for AOM and –2.10 mg/L (SD 4.99) for non-AOM; differences were not statistically significant (p≈0.24). At 3 months, mean change was +0.15 mg/L versus –0.14 mg/L (p≈0.66), and at 6 months –0.33 mg/L versus –0.19 mg/L (p≈0.90). Early fluctuations were observed, but sustained reductions were apparent at 12 months, particularly among participants achieving ≥10% weight loss.
Discussion
Participation in a structured hybrid obesity program led to reductions in systemic inflammation for both AOM and non-AOM participants, highlighting the effectiveness of comprehensive care. AOM participants exhibited consistent reductions across 12 months, while non-AOM participants also benefited, despite greater variability in individual responses. Differences between groups were not statistically significant at any timepoint, suggesting that the program itself—combining lifestyle, behavioral, and optional pharmacologic interventions—supports inflammation reduction. Incorporating hsCRP monitoring allows clinicians to assess treatment response and optimize individualized care. Overall, these real-world findings support hybrid obesity care as a feasible approach for improving both weight and inflammatory outcomes in adults with obesity.
Conclusion
A 12-month hybrid obesity-care program effectively reduced hsCRP in adults with obesity, demonstrating that both pharmacologic and non-pharmacologic participants experienced improvements in systemic inflammation. Differences between groups were not statistically significant, supporting the value of multidisciplinary, integrated interventions in real-world settings for promoting long-term metabolic and inflammatory health.